Bonding in Cosmetic & esthetic dentistry
Cosmetic or esthetic dentistry is generally used to refer to any dental work that improves the appearance (though not necessarily the function) of a person's teeth, gums and/or bite. This era started with the great advancements in adhesive dentistry or mainly in due to the rapid advancements in the bonding technology which made is possible to achieve acceptable bond strengths of tooth color materials to natural teeth and restorations. There can be no clinic in present times where bonding agent is not used several times each day. Let us look and understand this bonding process has evolved. We also shed light on often confusing issue of different generations of bonding agents.
History of Bonding Agents
First and Second Generation
The first- and second-generation bonding agents used during the 1960s and 1970s did not recommend etching the dentin, but instead relied on adhesion to the attached smear layer. The weak bond strength (2MPa�6MPa) to the smear layer still allowed dentin leakage with clinical margin stain.
Third Generation
The third-generation systems of the 1980s introduced acid etching of dentin and a separate primer designed to penetrate the dentin tubules as a method to increase bond strength. These systems increased bond strength to dentin (12MPa�15MPa) and decreased dentin margin failure. With time, however, margin staining caused clinical failure.
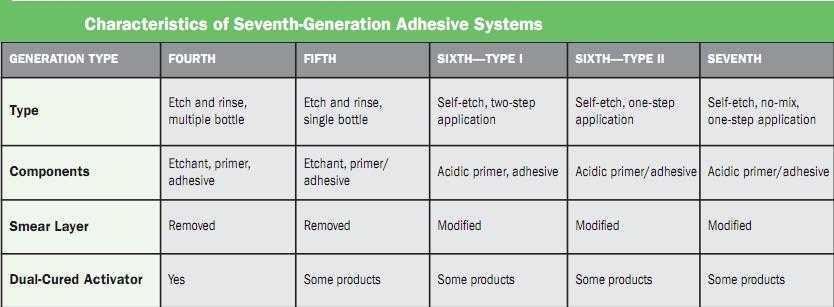
Fourth Generation
The fourth-generation adhesive systems of the early 1990s used chemistry that penetrated both etched and decalcified dentin tubules and dentin substrate, forming a �hybrid� layer of collagen and resin. Fusayama and Nakabayashi described the penetration of resin into dentin as giving high bond strengths and a dentin seal. In fact, Kanca introduced the idea of �wet bonding� with these systems. Products in this category include All-Bond� (Bisco), OptiBond� FL (Kerr), and Adper� Scotchbond� Multipurpose (3M ESPE). These bonding agent systems have the longest track record as far as research goes and they perform well clinically. In fact, OptiBond FL, an 18-year-old product, received the Product of the Year award from Reality magazine.8 Bond strengths for these adhesives were in the low- to mid-20MPa range and significantly reduced margin leakage compared to earlier systems. This system was very technique sensitive and required an exacting technique of controlled etching with acid on enamel and dentin, followed by two or more components on both enamel and dentin. Because of the complexity of multiple bottles and steps, dentists began requesting a simplified adhesive system. Fourth generation adhesive systems were very technique sensitive. Examples
- * 3M ESPE Adper Scotchbond Multi-Purpose Plus Adhesive System (BG)
- * ALL-BOND 3
- * Bond-It (BG)
- * DenTASTIC (BG)
- * LuxaBond Total Etch
- * OptiBond FL (BG)
- * ProBOND (BG)
Fifth Generation
To overcome the technique sensitive aspect was the main goal of developing the fifth-generation bonding systems, introduced during the mid 1990s, which combined primer and adhesive in one bottle while maintaining high bond strengths. Unit-dose packaging introduced during this era provided fresh chemistry for each procedure. Yet controlled etching, surface wetness, and resin placement continued to be a clinical challenge for some clinicians. These are still being used and give us very good bond strenths. Examples are
- * 3M ESPE Adper Single Bond Plus (abridged)
- * 3M ESPE Adper Single Bond Plus Dental Adhesive System (BG)
- * Admira Bond SD (BG)
- * ALPHA-BOND
- * Bond-1 (BG)
- * DenTASTIC UNO (BG)
- * DenTASTIC UNO�DUO
- * ExciTE (BG)
- * ExciTE DSC (BG)
- * ExciTE VivaPen
- * Gluma Comfort Bond + Densensitizer (PPL 2008)
- * IntegraBond (BG)
- * One Coat Bond (BG)
- * ONE-STEP (BG)
- * ONE-STEP PLUS (BG)
- * Prime & Bond NT (BG)
- * stae (BG)
- * TECO
Sixth Generation
The sixth-generation bonding systems introduced in the latter part of the 1990s and the early 2000s�also known as the �self-etching primers��were a dramatic leap forward in technology. The separate acid-etching step was eliminated by incorporating an acidic primer that was placed on the enamel and the dentin after tooth preparation. Several variations involved either mixing the acidic primer and adhesive before placement on the dentin and enamel, or leaving the primer on the tooth and then placing the adhesive over the primer.
These systems were also reported to reduce the incidence of post-treatment sensitivity found in previous systems. However, the bond strength to dentin and enamel is lower than fourth- and fifth-generation systems. Product in this category are
- * 3M ESPE Adper Prompt L-Pop Self-Etch Adhesive
- * 3M ESPE Adper Scotchbond SE
- * ACE ALL-BOND SE
- * AdheSE (abridged)
- * Brush & Bond (BG)
- * CLEARFIL LINER BOND 2V (abridged)
- * CLEARFIL SE BOND (2010 PPL)
- * CLEARFIL SE PROTECT (BG)
- * CLEARFIL SE PROTECT - Sensitivity Study
- * Contax (BG)
- * FL-BOND (BG)
- * FL-Bond II
- * frog (BG)
- * Futurabond NR (BG)
- * Futurabond NR SingleDose
- * GC UniFil Bond (BG)
- * Max Bond LC
- * One Coat Self-Etching Bond (BG)
- * One-Up Bond F Plus (BG)
- * OptiBond SOLO Plus (BG)
- * Prelude (BG)
- * Tenure Uni-Bond with Gloss-N-Seal (BG)
- * Xeno III (PPL 2008)
Seventh Generation Bonding
All-In-One is a single-component, self-etch adhesive that eliminates multiple steps when bonding direct and indirect restorations. Clinicians have everything they need for etching, priming and bonding in one material. These have been improving quality rapidly. Examples are
- * 3M ESPE Adper Easy Bond
- * AdheSE One (PPL 2008)
- * AdheSE One VivaPen
- * BeautiBond
- * BOND FORCE
- * Bond-1 SF Solvent Free SE Adhesive
- * CLEARFIL DC BOND
- * CLEARFIL S3 BOND - Microleakage Study
- * CLEARFIL S3 BOND - Sensitivity Study
- * CLEARFIL S3 BOND Single Dose (BG)
- * Futurabond DC
- * G-aenial Bond
- * G-BOND (PPL 2008)
- * go!
- * iBOND (BG)
- * OptiBond All-In-One
- * OXFORD BOND SE
- * Xeno IV (abridged)
- * Xeno IV Dual Cure
And Finally a composite that does not need bonding at all- call it SELF-ETCHING/SELF-BONDING composite
A self-adhering flowable composite combines the benefits of adhesive and composite technology into one product, bringing restorative techniques to new unprecedented heights. Simply syringe into the preparation, agitate, and light-cure. Immediately upon application it conditions, bonds, and seals without the need for an etchant or an adhesive. Two examples of this kind of product are
Fusio� Liquid Dentin from Pentron ClinicalVertise flow from Kerr.
Final words
In an excellent overview of factors that affect the bond strength of bonding agents, Powers et al point out that the type of substrate (ie, superficial dentin, deep dentin, permanent/primary dentition, carious dentin), phosphoric acid/acidic primers, preparation by air abrasion and laser, moisture, contaminants, desensitizing agents, and self-cured/light-cured restorative materials all affect the bond strength; bond strength is reduced by more than 50% when bonding conditions are not ideal.
Further, when lasers are used to prepare hard tissues, studies show that bonding to these surfaces may be more problematic than bonding to conventionally bur-prepared preparations.
Rushing to complete such procedures by reducing the priming time from 20 to 5 seconds can cause a 17% reduction in mean bond strength. In contrast, using a 20-second application time to agitate a self-etch adhesive significantly improves the shear bond strength to dentin. In addition to agitation, rather than applying a single coat of adhesive resin on dentin, up to four additional coatings increase the bond strength and decrease nanoleakage.
Multiple research reports attest to the existence of material incompatibilities that depend on formulation, and that bond strengths can be reduced by 45% to 90% or more when incompatible combinations are applied clinically.
Acetone-based adhesives show a high degree of technique sensitivity, and over- or under-drying the acid-etched dentin compromises the bond. Simplification of the bonding
procedure does not necessarily lead to improved bonding performance, especially in the long term. Alex perhaps has stated it best: �The bottom line is, it is incumbent on
every dentist to learn about their specific adhesive system, its idiosyncrasies, its strengths and weaknesses, and how to maximize its performance.�
Teeth Whitening Facts and Myths
Fiber reinforced composites in dentistry
Changing concepts in Class I and II cavity preparation
Latest Research On Dental Pain
Curing lights for composite resins
Fluorosis, epidemiology, indices and treatment
Lasers in Root canal treatment and Endodontics
Abfractions? How they are important in Restorative Dentistry
Caries Prevention in Children - The Indian Challenge
Mouth Rinsing before dental procedures.
Infection Control Routine for the Dental Clinic
Shade selection and Management
Obstructive Sleep Apnea- Do you know about it?
Genetically modified bacteria may prevent cavities - Put you out of Business?
A primer on all composite class materials
Options for esthetic restorations
Immediate and Early loading of Implants
Placement of gingival restorative margins
Bonding for the New Millennium
Access Cavity Preparation - Molars
Restoration of endodontic teeth
New cavity-fighting agent shows promise
Tooth Loss Linked to Pancreatic Cancer in Smokers
2-min brush helps achieve cleaner teeth: Study
Gum disease raises death risk in diabetics: study
Brushing Right After Drinking Soda may Harm Teeth
Benefits of Pre-procedural mouth rinsing?
To Bond Or not to Bond Amalgam