Fraudulent Use of Digital Radiography, and Microimplants
Fraudulent Use of Digital Radiography: Methods To Detect and Protect Digital Radiographs
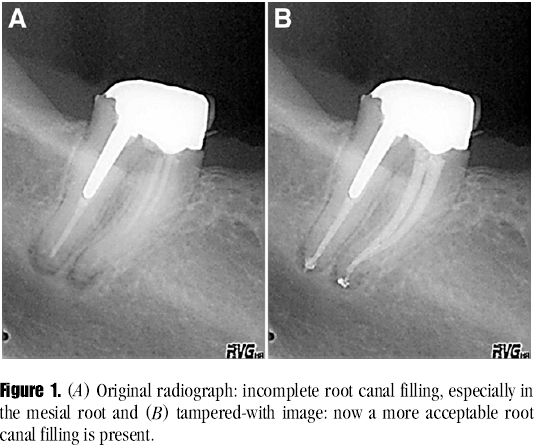
This very important article is published in Journal of Endodontics, May 2008 issue. As the use of digital radiography is becoming commonplace in dental clinics, it is better to be educated on these issues rather then being fooled by some computer savvy dentists who may show you great cases in their jazzy presentations.
To improve vision and diagnosis, dental x-ray software allows image enhancement (eg, adjusting color, density, sharpness, brightness, or contrast). Exporting digital radiographs to a file format compatible with commercial graphic software increases chances that information can be altered, added, or removed in an unethical manner.
Dental radiographs are easily duplicated, stored, or distributed in digital format. It is difficult to guarantee the authenticity of digital images, which is especially important in insurance or juridic cases. Image-enhancement features applied to digital radiographs allow mishandling or potential abuse. This has been illustrated by several recently published studies. A standard authentication procedure for digital radiographs is needed. A number of manipulated radiographic images are presented to show concerns about security, reliability, and the potential for fraud. Antitampering techniques and methods of detecting manipulations in digital medical images are discussed. See the pic above, one example of manipulation. To request full paper email to icdr@hotmail.com
Evaluation of the risk of infection through exposure to aerosols and spatters in dentistry
Aerosols in clinic can be dangerous ? American Journal of Infection Control May 2008 issue.
Many dental procedures produce extensive aerosols and splatters that are routinely contaminated with microorganisms.
Methods
Air containing blood-bearing aerosols and surfaces contaminated by sedimenting blood particulate was sampled in 5 different dental cubicles. To assess contamination by blood particulate, the concentration of hemoglobin (Hb) in the air and on the sedimentation surfaces was determined.
Results
The mean concentration of Hb in the air aspirated in the 5 cubicles was 0.14 ± 0.23 μg/m3, corresponding to a blood volume of 8.7 × 10-4 μL/m3. Similarly, the mean concentration of blood particulate sedimented on surfaces was calculated and found to be 1.56 μL/m2. In 80% of the cubicles monitored, 100% positivity to the Hb determination test was recorded in all of the surface samples.
Conclusions
The results obtained revealed contamination of both air and surfaces by blood particulate. Moreover, with the exception of those obtained in 1 cubicle, all of the samples of sedimenting particulate analyzed were positive for the presence of Hb.
Microimplants are here to stay, have you started using ? Come Try now DO IT NOW
Comparison of the intrusion effects on the maxillary incisors between implant anchorage and J-hook headgear --AJODO May 2008, Toru Deguchi etal
Introduction: Recently, miniscrews have been used to provide anchorage during orthodontic treatment, especially for incisor intrusion. Miniscrews during incisor intrusion are commonly used in implant orthodontics. Traditionally, effective incisor intrusion has been accomplished with J-hook headgear. In this study, we compared the effect of incisor intrusion, force vector, and amount of root resorption between implant orthodontics and J-hook headgear. Methods: Lateral cephalometric radiographs from 8 patients in the implant group and 10 patients in the J-hook headgear group were analyzed for incisor retraction. The estimated force vector was analyzed in the horizontal and vertical directions in both groups. Root resorption was also measured on periapical radiographs.
Results: In the implant group, significant reductions in overjet, overbite, maxillary incisor to palatal plane, and maxillary incisor to upper lip were observed after intrusion of the incisors. In the J-hook headgear group, significant reductions in overjet, overbite, maxillary incisor to upper lip, and maxillary incisor to SN plane were observed after intrusion of the incisors. There were significantly greater reductions in overbite, maxillary incisor to palatal plane, and maxillary incisor to upper lip in the implant group than in the J-hook headgear group. Estimated force analysis resulted in significantly more force in the vertical direction and less in the horizontal direction in the implant group. Furthermore, significantly less root resorption was observed in the implant group compared with the J-hook headgear group. Conclusions: The maxillary incisors were effectively intruded by using miniscrews as orthodontic anchorage without patient cooperation. The amount of root resorption was not affected by activating the ligature wire from the miniscrew during incisor intrusion.
Evaluation of orthodontic mini-implant anchorage in premolar extraction therapy in adolescents
AJODO, May 2008
Introduction: The purpose of this study was to determine the success rate, positional stability, and patient evaluation of orthodontic mini-implants (OMIs). Methods: Thirteen patients (8 girls, 5 boys; average age, 14 years 10 months) were treated with 82 OMIs measuring 1.6 mm in diameter and 6 mm in length placed in the buccal alveoli (1 unloaded OMI and 1 loaded OMI per quadrant). The right or left side of each arch was randomly selected for immediate loading with up to 250 g of direct force; the contralateral side was loaded 3 to 5 weeks later. Serial impressions, clinical observations, and orthodontic maintenance were performed until adequate space closure was achieved.
Results: The overall OMI success rate was 70.73%. As calculated with a mixed-model analysis, there was no statistically significant difference between the success rates of immediately loaded OMIs (80.0%) and delayed loaded OMIs (80.95%). The combined success rate for loaded OMIs (80.49%) was significantly higher than that of unloaded OMIs (60.98%). Patients' motivation for OMI treatment was primarily the desire to avoid headgear. Using a 100-mm visual analog scale, the patients indicated average scores of 54.77 for the amount of pain during OMI placement and 27.10 for the amount of pain during OMI removal.
Conclusions: OMIs are a predictable, effective, and well-tolerated anchorage source for adolescents. Neither the timing of force application nor the force itself precipitated failure of the OMIs. Orthodontic forces can be applied immediately to OMIs. Various anatomic and behavioral conditions unique to adolescents and a clinical learning curve can affect the success rate of OMIs.
posted by Healthmantra at
12:15 AM
![]()
![]()

0 Comments:
Post a Comment
<< Home